45 yr old patient with pulmonary tb
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box
CASE:
A 45 year old female patient came to OPD with chief c/o fever since 10days, cough and breathlessness since 5 days,no palpitations,no chest pain o up by Drr chest tightness,no h/o hemoptysis,complains of weightloss 5kgs during 2 months.Had 1 episode of vomiting and 4 episodes of loose stools yesterday
HISTORY OF PRESENT ILLNESS:
Patient was apparently asymptomatic 10 days back from when she had fever which is associated with chills and rigors,high grade ,intermittent and with diurnal variation,increasing during night and subsided by day.Cough is not productive and occasional.Breathlessness insidious onset and MMRC grade 3 associated with wheeze
No complaints of chest pain,palpitations,giddiness,hemoptysis,
1 episode of vomiting since yesterday-non projectile non bilious had food particles
4 episodes of loose stools since yesterday
PAST HISTORY:
No similar complaints in the past.Not a known case of DM,Htn,epilepsy,TB,CAV,CAD
PERSONAL HISTORY:
Mixed diet
Sleep and apettite normal
Bowel and bladder movements are regular
FAMILY HISTORY:
Not significant
GENERAL EXAMINATION:
On examination patient is conscious,coherent and cooperative.
PR:- 83 bpm
BP:- 130/90 mm hg
RR:- 16 bpm
Temp:- aferbrile
RS :- .BAE +
B/l crepts +
CVS :- S1 S2 +
CNS.:- NFND
P/A: - Soft,Nt
SYSTEMIC EXAMINATION:-
Patient was moderately built and nourished
No pallor,icterus,cyanosis,clubbing,koilonychia,lymphadenopathy,Edema
RESPIRATORY SYSTEM:-
Inspection:-
Upper respiratory tract:-
No sinus tenderness,no flaring of alar nasi,no nasal septal deviation,Throat and tonsils normal,no good oral hygiene
Lower respiratory tract:-
On inspection
Elliptical shaped chest,
Trachea- appears to be in midline
No supraclavicular hollowing
Infraclavicular flattening
No shoulder drooping
No kyphoscoliosis,no lordosis
Chest movements appears to be b/l symmetrical
No visible scars/sinuses/dilated veins,no intercostal retractions or swellings
On palpation :-
Trachea confirmed to be central in position
Apex beat- 1 cm medial to mid clavicular line in lt 5th intercostal space
Chest movements- b/l symmetrical
Vocal fermitus-b/l normal
No rib crowding/bony tenderness
Measurements:-
Ap diametre :- 7.5 inches
Transverse diametre:- 8 inches
Chest expansion 2 cm
Percussion
Decreased resonance on mammary and infrascapular areas
On auscultation
Breath sounds:- nrml vesicular breath sounds
Crepts in mammary and infra scapular areas of both lungs
Wheeze (-)
Rhonchi(-)
Decreased breath sounds on mammary area of rt lung
INVESTIGATIONS
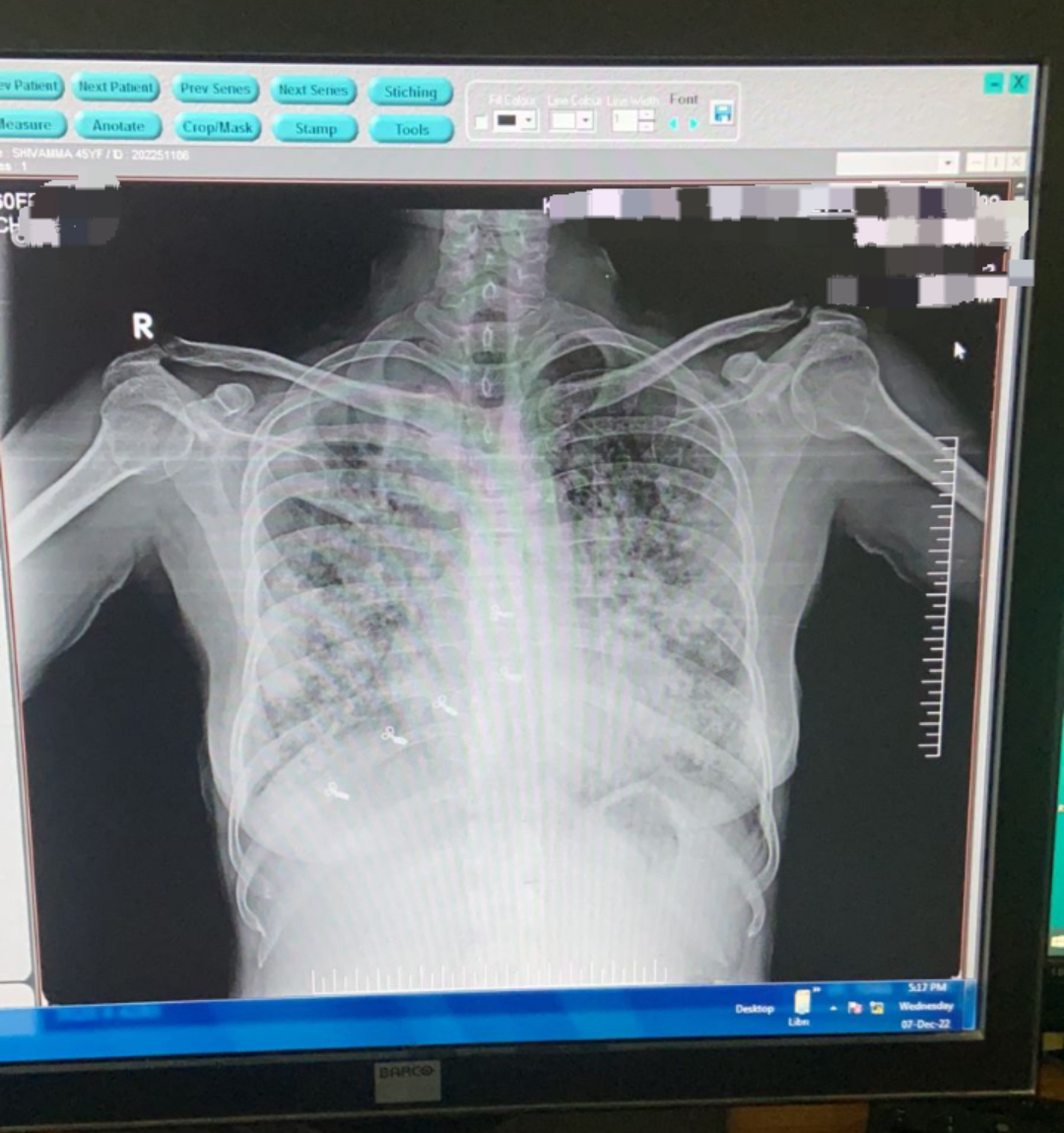
Chest x ray

Usg abdomen

Hb-8.2
TLC- 29000
PLT-3.2
N-92
L-03
M-04
E-01
PCV-24.6
MCV-68.3
MCH-20.0
MCHC-29.3
RDW-18.7
RBC-3.60
Color doppler:-



Sputum culture- tested negative for AFB
CBNAAT:- tested positive for AFB
Provisional diagnosis:-
Septic shock secondary to pneumonia
? Tuberculosis infection
posted by Sri Govardhini @ December 29, 2022
![]()
